Two weeks ago, RIJ reported that the Financial Research Corporation had described as a “myth” a 2006 estimate by the Employee Benefit Research Institute that the average 65-year-old couple would need about $300,000 in savings just for out-of-pocket medical care in retirement.
The report instantly provoked the ire of EBRI’s president, Dallas Salisbury, who said that calling EBRI’s numbers a myth was tantamount to calling them lies. EBRI researcher Paul Fronstin also noted that FRC’s own data actually supported EBRI’s conclusions.
Each of these responsible organizations has a legitimate point. The EBRI has solid evidence regarding the amount of savings a retiree will need to pay for the health insurance needed to supplement Medicare and to pay out-of-pocket health care costs over the average life expectancy.
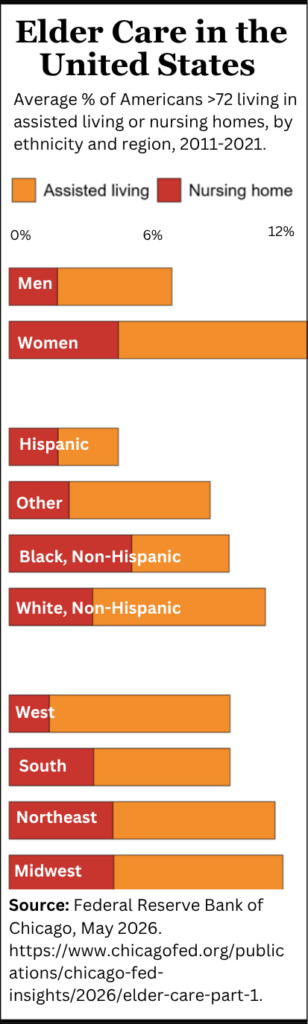
If you factor in health care cost inflation, the amount of savings needed for maximum protection becomes a shocking number. In a report last summer, EBRI estimated that when today’s 55-year-olds retire in 10 years, the men would need between $114,000 and $634,000 to cover insurance and medical other costs in retirement.
For women, the estimates are even higher. The average 55-year-old woman will need $164,000 to $754,000 in savings to cover medical expenses during retirement. Each person’s spending would depend on individual experience and whether he or she wanted a 50%, 75% or 90% chance of covering all health care costs in retirement, the EBRI said.
And that’s not counting eye care, dental care, or the potential cost of nursing home care, which now averages about $69,000 a year.
But the FRC also had a point. You can calculate prices, but people won’t necessarily be able to pay them. The savings requirements for health care may be mythical in the sense that very few Americans are on track to save anywhere near those amounts, or to have a retirement income that can support that level of expenditure. And if they can’t save or spend that much, they won’t.
Hence the conclusion the EBRI projections are unrealizable and therefore “mythical.” The EBRI projections may show the average costs—but that doesn’t mean the average person can or will pay them. People who can’t afford to be fully insured won’t be. Many will presumably find a way to survive.
“We’re not trying to dispel the idea that health expenses will be an important factor, and even $4,500 is not an insignificant amount,” he said. “But the idea that you need three hundred grand for health care or you’re not going to make it isn’t necessarily true.”
There’s actually little difference of opinion among the research groups. They all see health care costs rising astronomically. And they all acknowledge to some degree that straight-line projections based on current trends might not be literally predictive, because neither the government nor most individuals will be able to pay that much.
Richard Johnson of the Urban Institute and Jon Skinner of Dartmouth College use words like “implausible” and “unsustainable” to describe the burden of health costs on retirees in two or three decades.
“Herb Stein, the chairman of Richard Nixon’s Council of Economic Advisors, used to say that ‘unsustainable growth paths are unsustainable.’ And so if you believe that, EBRI’s point is well put,” said Skinner, who in 2008 co-authored with Kathleen McGarry a research paper entitled, “Out-of-Pocket Medical Expenses and Retirement Security.”
“If you’re 55 and you’re looking ahead to age 75, and health care costs continue to rise by four percentage points per year higher than inflation, then there’s obviously a big expense coming your way,” he said. “It’s the private equivalent of what’s happening on the public level [with Medicare]. If health care costs rise 4% a year then the government will be underwater too.”
“If you accept the Congressional Budget Office projections of future budget deficits, then there’s nothing on the landscape that shows that the growth will stop. As for the EBRI’s number, it’s just a number. It’s illustrative. The basic point is that over the long term out-of-pocket spending for health care is going to be a lot of money.
“I interpret EBRI’s numbers to mean that you better start saving more or plan to reduce other forms of consumption. You can’t save for every contingency. The message is that you must prepare for it,” he said, adding that the Obama administration’s “health care reform won’t change much in the short term. It will be a decades-long process to reform the incentives in our [health care] system.”
In their paper, Skinner and McGarry wonder “whether these doomsday predictions are overblown,” given the shortage of surveys of actual retiree out-of-pocket health care spending.
Their study suggests two reasons why predictions are difficult to make. For one thing, “expenditures [are] skewed towards the very end of life, with more than one-third of the expenditures in the last year coming during the last month of life,” they point out.
Second, people tend to spend more when they have more to spend. “Wealth is more predictive of spending on out-of-pocket health care expenditures than the flow of income,” they write. People with more money can and do spend it on things like in-home elevators and other optional things that people with less money simply do without.
Another specialist in this area is Richard W. Johnson of the Urban Institute, who in October 2004 published a study with Rudolph G. Penner called “Will Health Care Costs Erode Retirement Security?” When asked about the EBRI’s figures, he said his estimates were somewhat lower.
“I get an estimate of more like $75,000 per person,” Johnson told RIJ, or $150,000 per couple. “That’s out-of-pocket health care spending from age 65 forward to death. That’s an average. The median would be lower. Some people will spend nothing because they’re on Medicaid.
“On the other hand, so many of the people who are fully insured are getting huge subsidies from their employers. Ten percent of the over-65 population will experience catastrophic costs, but the median person won’t necessarily spend much.
“Even though my numbers are not as high as EBRI’s, they underscore the need to control spending,” Johnson added. “If [health care spending] continues at its current rate it will bankrupt the government and a lot of families.
“I think you’ll find that once individual spending gets too high, people will just cut back. They will become more savvy consumers. They won’t get those extra tests. That will bring down spending to some extent. But the numbers highlight the fact that health care will be expensive. And even if you’re fortunate enough to have [employer-sponsored] retirement coverage or expect it in the future, you shouldn’t rely on it entirely because it might disappear.”
Out-of-pocket health care expenses in retirement will fall most heavily on people who are in the so-called second income quintile—the lower middle class—who earn too much to qualify for Medicaid. Johnson’s research showed that health care costs might consume half of their after-tax income. Hut he called that scenario “implausible” and wrote, “It is doubtful that society would tolerate this result.”
© 2009 RIJ Publishing. All rights reserved.