As the world grapples with the growing COVID-19 (coronavirus) threat, a useful reference point is the Spanish Flu of 1918. Given what we now know about COVID-19, are we looking at something of similar severity to the Spanish Flu, or materially less severe, or perhaps worse?
Up until now, the Spanish Flu has been generally regarded as a “worst case” reference point in pandemic modeling: This is as bad as it could get.
The thinking would be that healthcare is so much more advanced now, and we are not recovering from four years of strategic war as was the case then. These positive factors should more than compensate for the (then unimaginable) extent of international air travel and globalization of trade. But perhaps that rationale no longer holds, and we could be heading for something similar.
Plausible mortality impacts

Matthew Edwards
An actuary’s immediate reaction to COVID-19 is, of course, to model it. But even now, with more than two months of data, there are considerable obstacles to any plausible modeling using the typical pandemic modeling methods (e.g. the ‘SIR’ approach of splitting people into the states of susceptible, infected, and recovering, with age/gender-specific transition rates) and this article does not attempt any such modeling.
Most pandemic models involve a “spread” assumption, R0, which represents how many individuals an infected person will transmit the virus to (in an otherwise perfectly susceptible population). An R0 parameter of one, for instance, equates to a stable state; a value greater than one (at the start of an outbreak) implies growth in infections, with the potential for exponential growth in the absence of interventions. Normal influenza spread implies a parameter of two to three whereas measles is one of the most contagious viruses with an R0 of 12 to 16.
At the moment, even this fundamental element is uncertain by a wide range. Various publications so far have it ranging from 1.4 to over six, while even the World Health Organization’s (WHO’s) suggested range allows almost 100% variation (from 1.4 to 2.5).
In addition, as a further complication, the effective rate of reproduction will differ between countries and also vary over time as people shift their routines to avoid infection (hopefully decreasing as people and governments become more aware of the problems).
Then we have the problem of mortality, the case fatality rate (CFR), which measures the mortality of infected cases. Overall estimates are around 2%, but here there is wide variation between the experience in Wuhan (above 5%) and outside that area (of the order of 0.7%). Reporting and data issues add further uncertainty; even determining the number of cases is challenging, especially given the asymptomatic cases whose number cannot accurately be measured.
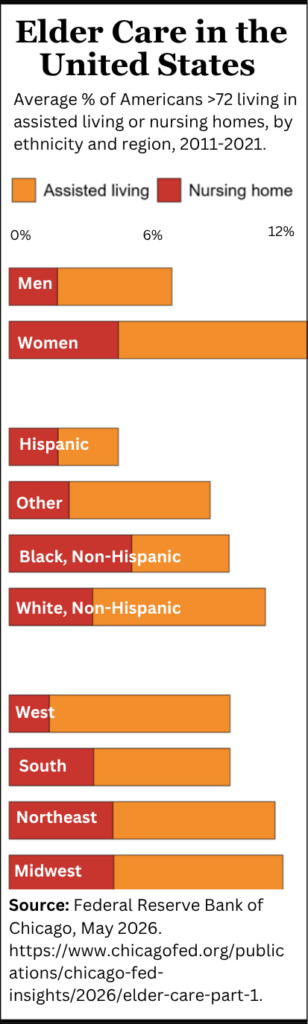
These figures compare with the following reference points:
The overall CFR in any country is likely to be heavily influenced by the availability of appropriate healthcare resources. However, the age variability seen so far is likely to be similar across countries.
The Chinese experience showed mortality rates varying broadly and exponentially by age, from circa 0.2% for ages up to 40, increasing to 4% for the 60 to 69 age band, 8% for the next decade of age, and roughly doubling again to 15% for anyone 80 or older. (This concentration of deaths at higher ages is supported by observation of the ages of reported European fatalities.)
So what sort of impact is plausible? To paint a very broad picture, if we assume a CFR in the 0.5% to 1.0% range (in line with the ‘outside Hubei’ COVID-19 figures to date, and the 1957/68 pandemics), this could lead to, as a plausible order-of-magnitude conjecture, a doubling of mortality in a country such as the U.K. for a period of several months. That is, an overall doubling of population mortality, not a doubling of mortality for infected cases. This would be a bad outcome (and is not a ‘best estimate’ prediction), but it is plausible.
Moreover, the above broad-brush perspective deliberately overlooks various likely and material indirect impacts. The likely surge in patient volumes at healthcare facilities related to a sustained COVID-19 outbreak in any country could mean a corresponding squeeze on access to care (and hence, increased mortality) for patients already suffering from other serious conditions in secondary care. There will be an equivalent but less severe effect at the primary care level.
Quarantine and self-isolation will also have a detrimental effect on those suffering from chronic conditions at home. The healthcare workforce will itself be depleted by absences. Furthermore, supplies of medicine taken for granted will potentially be adversely affected by production supply chain issues.
There is one material mitigating point from an insurance perspective, if not from that of the individuals affected: the coronavirus will disproportionately affect the less healthy (in particular, people already with chronic conditions), and hence the mortality impact does not consist entirely of ‘new’ deaths but will include a material proportion of ‘accelerated’ deaths (hence leading to correspondingly reduced mortality in later years).
A more positive point for insurers is the opportunity for innovative product design in the face of a very clear set of consumer concerns. By way of example, Generali announced in February a new product aimed specifically at providing coronavirus cover for healthcare costs and loss of earnings; other major insurers have launched similar products.
Impacts for insurers
The variability of the mortality impact by age makes the impact highly variable by type of insurer. Clearly, annuity writers will experience an unusually high mortality year (even under the more benign scenarios). Protection writers will see a mortality impact likely to be of similar order of magnitude to their capital allowance for life cat risk (for example, the Standard Formula of Solvency II sets this at 1.5 per mille, and internal model firms will have generally similar calibrations); the major question for them is the extent of their reinsurance.
The main losers will be firms with large whole of life books but low levels of reinsurance: there is likely to be a large amount of sum at risk for policyholders in their 50s and 60s, with a material mortality impact from the COVID-19 outbreak.
However, there are a range of other impacts that insurers with well-developed risk management functions and capital models should already be prepared for (one silver lining of the COVID-19 problem is that it does focus minds on real-life examples of complex interacting risks stemming from just one driver).
Asset markets are clearly badly affected, with (by way of example) the FTSE-100 down 12.7% and the S&P 500 down 8.6% from January 1 to February 28 this year. Operational risk will be a concern, with firms needing to prepare for significant staff absences, and absences in their suppliers (third-party outsourcers will not be “immune” to the problem themselves).
Occurring as this outbreak has immediately after most firms’ year-end means that insurers will have a couple more months to wait and see before finalizing their revised assumptions for mid-year reporting. By this time, mortality assumptions are likely to need increasing, probably with a short-term adjustment, while annuity writers might find it reasonable to wait and see as far as base assumptions go, noting that they can be fairly aggressive this year with improvement assumptions.
For instance, in the U.K., this is likely to mean no insurer will want to move to the latest mortality projection model CMI_2019, which gives slightly higher life expectancies than the previous versions. (In theory, the proper approach would be to combine a short-term adjustment to base tables with incorporation of CMI_2019, allowing for greater life expectancy for survivors. In practice, the uncertainties that will persist until even end 2020 will likely mitigate against this approach.)
In an ideal world, actuaries would wait for near-certainty before changing any major assumptions. In the first half of 2020, such an approach is unfortunately not feasible.
© 2020 WillisTowersWatson. Used by permission.